
Sometimes an opportunity is about invention. Sometimes it's about timing. India may be entering one of those rare windows where timing does an unreasonable amount of the work.
Not because India has "solved healthcare" (it hasn't), but because digital rails are emerging that can reduce the biggest hidden tax in digital health: fragmentation.
Remote patient monitoring doesn't fail mainly because sensors are weak. It fails because identity is messy, records are scattered, provider trust is uneven, and interoperability is expensive. In many markets, startups spend years just stitching pipes together.
India now has a chance to move differently.
ABDM is explicitly aimed at interoperability and longitudinal digital health infrastructure—building the backbone for connected health data and enabling a longitudinal record for citizens. Ministry of Health and Family Welfare Public-facing ABDM resources outline the ecosystem components and documentation for different stakeholders. Ayushman Bharat Digital Mission Academic analysis of ABDM also describes ABHA as a mechanism for patient identification/authentication within this ecosystem.
Why does that matter for RPM?
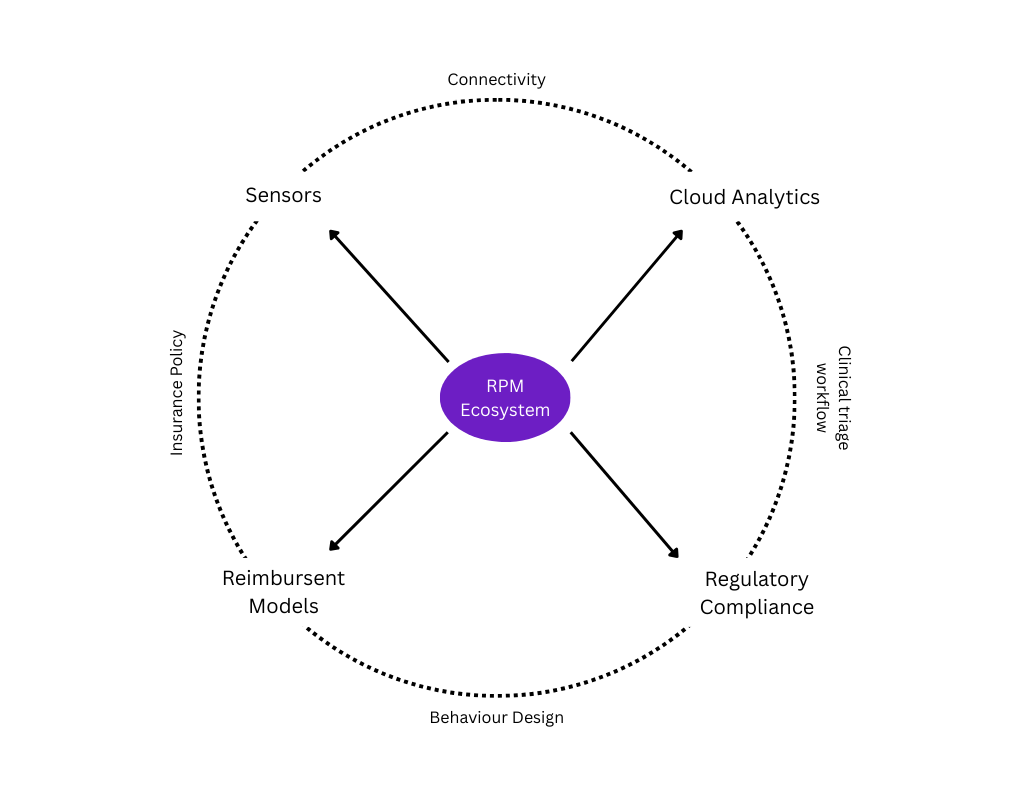
Fig 1.0 — Remote Patient Monitoring Flywheel
Because RPM becomes dramatically more valuable when monitoring is not trapped inside a single app or vendor silo. Identity + portability + provider verification + interoperable workflows can convert "device data" into "care continuity."
Add to this two reality engines:
- A massive chronic care burden that benefits from continuous supervision instead of episodic rescue.
- Normalization of remote follow-up behavior post-COVID, which makes ongoing monitoring programs less culturally weird and more operationally feasible.
This is why the "unfair advantage" framing isn't hype. The structural ingredients for leapfrogging are here: new digital rails, massive demand, and a cost-sensitive environment that rewards outcome and efficiency over shiny tech.
But the advantage is not automatic.
India's digital health moment will be wasted if products treat ABDM like a badge rather than a design principle. The winners will build as if interoperability is default, continuity is assumed, and care workflows (not dashboards) are the unit of value.
India doesn't need to repeat every dead end that other markets took. It can compress the journey—if builders prioritize connected care over disconnected apps.